Free Shipping on orders over $99
 888-616-4156
888-616-4156 

Numbness, tingling, and pain in the hand and forearm are caused by pressure on the median nerve in the wrist, resulting in carpal tunnel syndrome. Typically, the symptoms worsen over time, and if left untreated, it can result in permanent hand dysfunction, including sensory loss in the fingers and weakness. Timely diagnosis and treatment are crucial to prevent long-term complications associated with carpal tunnel syndrome.
Early symptoms can often be relieved with simple measures like:
*Using a wrist splint during sleep.
*Engaging in exercises to maintain nerve mobility.
*Steering clear of activities that worsen your symptoms.
*Injecting steroids into the carpal tunnel.
Continued pressure on the median nerve can result in nerve damage and worsening symptoms. To prevent permanent damage, surgery may be recommended for certain patients to alleviate pressure on the median nerve.
Anatomy
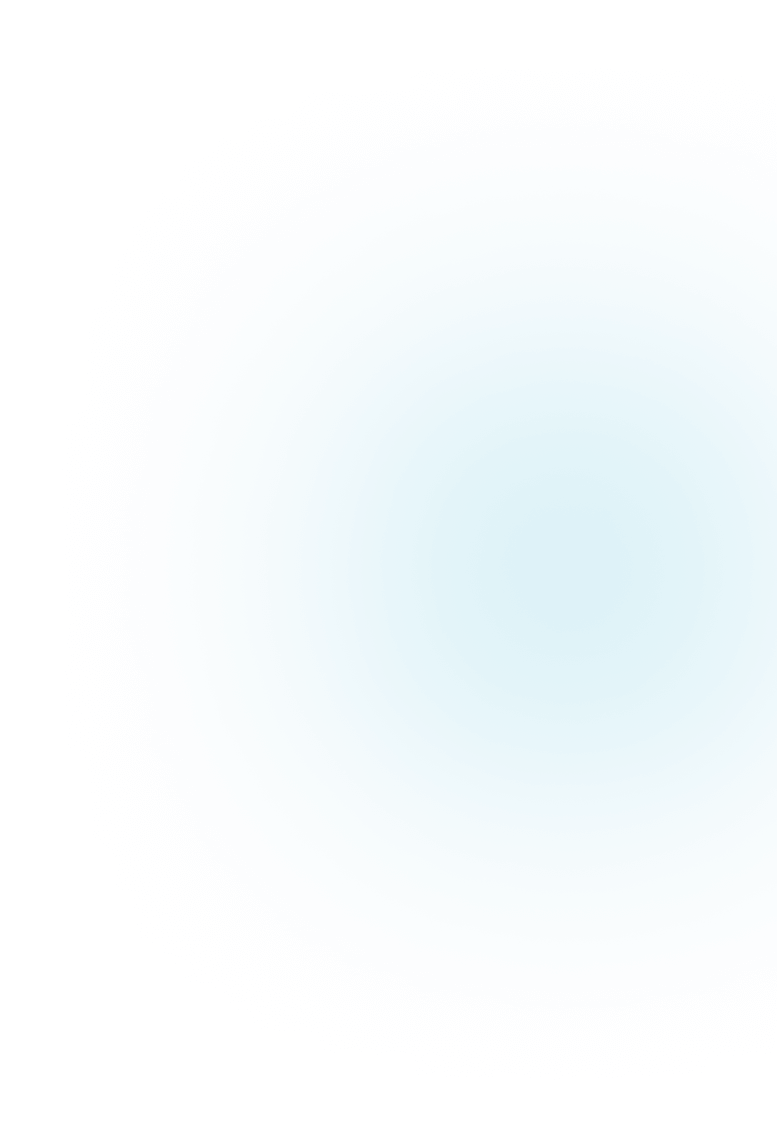
The carpal tunnel, approximately one inch wide, is a narrow passage in the wrist. Comprising the floor and sides of the tunnel are small wrist bones known as carpal bones.
The carpal tunnel is confined by a sturdy band of connective tissue known as the transverse carpal ligament, forming its rigid boundaries, limiting its stretch or size expansion.
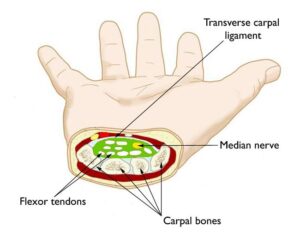
Originating as a group of nerve roots in the neck, the median nerve consolidates into a singular nerve in the arm. It courses down the upper arm, traverses the elbow, enters the forearm, and passes through the carpal tunnel at the wrist en route to the hand and fingers. The nerve divides into smaller branches, especially in the palm, providing sensation to the thumb, index finger, middle finger, and half of the ring finger (thumb side).
Additionally, the median nerve governs the muscles around the base of the thumb. Accompanying the nerve through the carpal tunnel are nine tendons responsible for bending the fingers and thumb, aptly named flexor tendons.
Description
The onset of carpal tunnel syndrome occurs when the tunnel narrows or when the synovium, the tissue encompassing the flexor tendons, swells. This swelling exerts pressure on the median nerve, diminishing its blood supply. The abnormal pressure on the nerve manifests as sensations of numbness, tingling, pain, and weakness in the hand.
Cause
A blend of factors typically contributes to most cases of carpal tunnel syndrome. Research indicates a higher likelihood of the condition in women and older individuals.
Other risk factors for carpal tunnel syndrome include:
*Genetics play a crucial role, with heredity being a significant factor. Some people naturally inherit a smaller carpal tunnel or have anatomical differences that affect the nerve space. These traits can run in families.
*Engaging in repetitive hand use, where the same motions or activities are repeated over an extended period, can exacerbate wrist tendons, leading to swelling that applies pressure on the nerve.
*The position of the hand and wrist during activities is crucial. Prolonged engagement in activities that entail extreme flexion or extension of the hand and wrist can elevate pressure on the nerve.
*Pregnancy can lead to hormonal changes that induce swelling, putting pressure on the nerve.
*Certain health conditions such as diabetes, rheumatoid arthritis, and thyroid gland imbalances are linked to carpal tunnel syndrome.
Symptoms
Symptoms of carpal tunnel syndrome may include:
*Sensations of numbness, tingling, burning, and pain, especially in the thumb and the index, middle, and ring fingers, frequently disrupt sleep, waking individuals up at night.
*Intermittent sensations resembling shocks that extend to the thumb, index, middle, and ring fingers.
*Discomfort or tingling that might extend up the forearm towards the shoulder.
*Weakness and lack of coordination in the hand, potentially hindering precise movements like buttoning clothes.
*Dropping objects may occur due to weakness, numbness, or a diminished sense of proprioception (awareness of your hand’s position in space).
Typically, carpal tunnel syndrome symptoms develop gradually without a specific injury, with initial occurrences being intermittent. As the condition progresses, symptoms may become more frequent or persistent. Nighttime symptoms are prevalent, often awakening individuals due to wrist bending during sleep. Daytime symptoms often manifest when holding something for an extended period with the wrist bent, such as while using a phone, driving, or reading. Some patients discover that moving or shaking their hands provides relief from symptoms.
Treatment
While the progression of carpal tunnel syndrome is gradual, it tends to worsen over time without intervention. Therefore, early evaluation and diagnosis by a doctor are crucial. In the initial stages, it might be possible to impede or halt the disease’s advancement.
Nonsurgical Treatment
When identified and addressed in its early stages, carpal tunnel syndrome symptoms can frequently be alleviated without resorting to surgery. If there is uncertainty in the diagnosis or if symptoms are mild, your doctor will initially suggest non-surgical treatments.
Nonsurgical treatments may include:
*Bracing or splinting. – Wearing a brace or splint during the night prevents bending of your wrist while sleeping. Maintaining your wrist in a straight or neutral position minimizes pressure on the nerve within the carpal tunnel. Using a splint during the day, especially during activities that worsen your symptoms, can also be beneficial. At Daphco Medical Equipment, we also offer various types of wrist/finger splint braces which can alleviate pain and provide support. Click this link to see our full list of wrist braces or if you are a Medicare beneficiary, fill out this form on how to get the brace with your Medicare insurance.

*Nonsteroidal anti-inflammatory drugs (NSAIDs). – Anti-inflammatory medications such as ibuprofen and naproxen can help relieve pain and inflammation.
*Activity changes. – Symptoms often occur when your hand and wrist are in the same position for too long — particularly when your wrist is flexed or extended. If your job or recreational activities aggravate your symptoms, changing or modifying these activities can help slow or stop progression of the disease. In some cases, this may involve making changes to your work site or workstation.
*Nerve gliding exercises. – Some patients may benefit from exercises that help the median nerve move more freely within the confines of the carpal tunnel. Specific exercises may be recommended by your doctor or therapist.
*Steroid injections. – Corticosteroid, or cortisone, is a potent anti-inflammatory agent that can be administered into the carpal tunnel. Such injections frequently alleviate painful symptoms or assist in calming a flare-up of symptoms.

-For individuals with mild, early-stage disease, injections may provide long-term relief of symptoms.
-In individuals with moderate to severe disease, the beneficial effects of the injection may be temporary.
A cortisone injection may also be utilized by your doctor as a diagnostic tool to help identify your carpal tunnel syndrome.
Surgical Treatment
If nonsurgical treatments fail to alleviate your symptoms or offer only temporary relief, your doctor may suggest surgery.
The decision of whether to recommend surgery is based on:
*The intensity of your symptoms.
*Findings in your physical exam
*Unresponsive to non-operative treatments
*Testing results
In cases where there is persistent numbness and muscle wasting in the thumb or when non-operative treatments do not provide relief, surgery may be recommended to prevent irreversible damage. Additionally, significant nerve changes on testing may indicate the need for surgery.
Surgical Procedure
The surgical procedure conducted for carpal tunnel syndrome is known as carpal tunnel release. While there are two primary surgical techniques, both aim to alleviate pressure on the median nerve by cutting the ligament forming the tunnel’s roof (transverse carpal ligament). This release enlarges the tunnel, reducing pressure on the median nerve and facilitating proper blood flow and nerve function.
In the majority of cases, carpal tunnel surgery is performed on an outpatient basis. The procedure can be conducted under general anesthesia, inducing sleep, or under local anesthesia, numbing only the hand and arm. In instances with local anesthesia, a light sedative may be administered through an intravenous (IV) line inserted into a vein in your arm.
Open carpal tunnel release. – In an open carpal tunnel release surgery, a small incision is made in the palm of the hand, providing visual access to the inside of the hand and wrist. During the procedure, the transverse carpal ligament (roof of the carpal tunnel) is divided by the doctor, enlarging the tunnel and alleviating pressure on the median nerve. Post-surgery, the ligament may gradually grow back in a lengthened manner, creating more space in the carpal tunnel and relieving pressure on the median nerve.
Endoscopic carpal tunnel release. – During endoscopic surgery, your doctor creates one or two smaller skin incisions known as portals and employs a miniature camera (endoscope) to visualize the inside of your hand and wrist. Using a special knife, the transverse carpal ligament is divided, mirroring the process in the open carpal tunnel release procedure.

The outcomes of both open surgery and endoscopic surgery are comparable, with each technique having its own set of benefits and potential risks. Your doctor will discuss with you the most suitable surgical approach based on your individual circumstances.
Recovery
Following the surgery, you’ll be advised to elevate your hand above your heart and engage in finger movements to minimize swelling and prevent stiffness.
Post-surgery, you can anticipate experiencing some pain, swelling, and stiffness. Mild soreness in your palm may persist for several weeks to months.
For most patients, nighttime symptoms show significant improvement within the initial week after the surgery.
Grip and pinch strength
Search Articles
Latest Articles

 28th Feb, 24
28th Feb, 24
 28th Feb, 24
28th Feb, 24 
- 23rd Feb, 24
- 20th Feb, 24
- 15th Feb, 24

- 13th Feb, 24